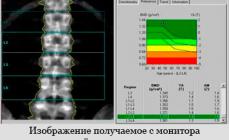
Scoliosis is the lateral curvature of the spine, which is localized in the chest, cervical or lumbar department. It is considered one of the most common diseases of the spine.
Fig.1 X-ray computer tomogram of a skeleton at a junior dysplastic scoliosis
general information
The curvature form is divided into a simple (C-shaped) scoliosis at which the spine is shifted only in one direction, complex (S-shaped), when the curvatures are somewhat and they are directed in different directions, and total (e--shaped), which is characterized by multiple curvature.
Scoliosis are dysplastic, traumatic, myopathic or neurogenic origin.
By types differ:
- Shainian chest scoliosis. The top of the spine curvature at 4-5 breast vertebrae. Accompanied by early deformations in the chest area and changes in the facial skeleton.
- Chest scoliosis. At the level of 8-9 breast vertebrae. The curvature is right and left-sided.
- Lumbar chest scoliosis. The vertex of the curvature of the first arc of the spine at the level of 10-11th breast verses.
- Lumbar scoliosis. At the level of 1-2 lumbar vertebrae. Progresses slowly, but early pain in the deformation area arise.
- Combined, or S-shaped scoliosis. It is characterized by two primary curvature arcs - at the level of 8-9 breast and 1-2 lumbar vertebrae.
In addition, the disease is also classified at the corner of the curvature measured according to the COBB method: with the first degree an angle of 1-10 °, the second - 11-25 °, the third - 26 ° -50 °, with the fourth - more than 50 °.

Fig.2 Measurement diagram of the magnitude of the scoliotic arc by COBB
Scoliosis can also be fixed and non-fixed, disappearing in a horizontal position, for example, when shortening one limb.
At the same time, the rotation around the vertical axis is usually observed with scoliosis. The rotation contributes to the deformation of the chest and its asymmetry, the internal organs are compressed and shifted.
The scoliosis of congenital, based on various vertebral deformations lie:
- underdevelopment;
- wedge-shaped form;
- additional vertebrae and. t. d.
Acquired scoliosis includes:
- rheumatic, arising usually suddenly and imagining muscle spasm on a healthy side in the presence of phenomena of myositis or spondylitrite;
- rachitic, which are very early manifested by various deformations of the musculoskeletal system. The softness of the bones and the weakness of the muscles, wearing a child in the hands (mainly on the left), a long-lasting seat, especially at school, - all this favors the manifestation and progression of scoliosis;
- paralytic, more often arising after children's paralysis, with one-sided muscular lesion, but may be observed with other nervous diseases;
- the usual, on the basis of the usual bad posture (often they are called "school", since at this age they get the greatest expression). The direct cause of them may be incorrectly arranged desks, scattering schoolchildren without taking into account their growth and numbers of the party, wearing portfolios from the first classes, holding a child while walking in one hand and. t. d.
Of course, not all kinds of scoliosis are covered by this list, but only basic.
Statistics of numerous studies to identify scoliosis in children indicate that this deformation is one of the most frequent diseases of the musculoskeletal system, which tends to progression and reaches the highest degree to the end of the growth of the children's body.
Heavy curvatures of the spine and chest significantly affect the functions of the internal organs:
- reduce the volume of pleural cavities,
- violate the mechanics of breathing, which, in turn:
- worsens the function of external breathing,
- reduces the saturation of arterial blood oxygen,
- changes the character of fabric respiration,
- causes hypertension in a small circulation of blood circulation,
- myocardine hypertrophy of the right half of the heart - the development of symptom complex of pulmonary heart failure, combined with the name "Kifoscoliotic heart"
The most dangerous time for the appearance of scoliosis is the periods of intensive growth of the child (6-8 years, 10-14 years), as well as the period of puberty (girls are 10-13 years old, boys are 11-14 years old). According to statistics, every second high school student suffers from this disease.
In about 80% of all cases, the cause of the occurrence of unknown is unknown. Such scoliosis is called idiopathic.
How to determine the presence of scoliosis?
Take the usual posture pose (stand up and relax). First of all, you should pay attention to the following main signs of scoliosis:

Fig.3 Patient 10 years with dysplastic scoliosis IY degree
- one shoulder slightly above another
- one of the blades went "Little" (repents the corner of the blade)
- different distance from the hands pressed against the side to the waist
- as a slope forward, the curvature of the spine is noticeable
If at least one of these signs found - go to the orthopedist, or, at least to the surgeon.
Treatment Scoliosis
Treatment depends on the age of the patient, the type of scoliosis and the degree of deformation of the spine.
Children's scoliosis at the I and II degrees of the spinal curvature are treated conservatively. An important condition for successful treatment is the full and rich in vitamin food, regular stay in the fresh air, moving games. The bed must be tough for which a wooden shield is placed on the bed. Chair and desk in the workplace must match growth. It is necessary to watch the child sitting at the table straight, and the feet at the same time reached the floor. The correct installation of light is also important, and when impaired vision, its correction is required.
Therapeutic physical culture is one of the auxiliary means of conservative treatment of scoliosis. Exercise has a stabilizing influence on the spine, strengthening the muscles of the body, allow you to achieve a corrective impact on deformation, improve the posture, the function of external breathing, give a common effect. LFC is shown at all stages of scoliosis development, but it gives more successful results with initial scoliosis forms.
Physical exercises that increase the flexibility of the spine and leading it to excellence.
In addition to the governing governments, a wellness, there are many special, for example, to strengthen the abdominal press muscles, chest, improving posture. These exercises allow to some extent to correct the flaws of the figure, allow you to better own your body.
Proper posture makes us not only more attractive, but largely contributes to the normal functioning of all organs and organism systems, is the prophylaxis of scoliosis. Success will depend on the duration and regularity of classes.
We systematically conduct therapeutic gymnastics, but with an increase in the deformation value, over 20 ° Cobb, the corset is prescribed.
Previously, conservative treatment was carried out in special boarding schools for children with scoliosis, in which simultaneously with training on the usual program, the necessary round-the-clock treatment regimen was created, which provided, for example, conducting training sessions in the situation.
Currently, the "golden" standard of conservative treatment is considered to be a cake cake (J. Cheneau). The corsets of this type are used in the treatment of children from 5 years and up to the completion of bone growth (up to 15-17 years). The longer wearing of the corset in persons who ended with bone growth, therapeutic effects has no. The main advantage of the corset corset except its high efficiency is the possibility of a child not to limit the game and motor activity during the wearing period: - only weight lifting is not allowed.




Fig.4 Patient K., 16 years old. Dysplastic scoliosis IY degree. Correction in the cake corset (in the picture).
Operational treatment is appointed with a significant and rapidly progressive scoliosis and is in the installation of various kinds of mechanical endocorrers that correct the curvature of the spine.
Surgery
The initial (initial) testimony for the operation varies depending on the age and psychological problems of the patient, localization and type of its curvature, school and experience of a specific surgeon, as well as the effectiveness of affordable corset treatment.
Indications for surildren with scoliosis are considered:
- The presence of a scoliotic arc of more than 40 °
- The presence of a progressive arc to an angle of more than 1 ° for more than 2 years
- The presence of pain syndrome
- The presence of neurological disorders
- Patient desire.
In operational treatment, the spine straightens up to a certain angle with the help of metal rods, which leads to immobilization of these spinal departments. The surgery during scoliosis is primarily suitable for strong curvatures that can no longer be treated by other methods. Operational fixation can prevent further progression and deterioration.
There are two main types of operations during scoliosis: rear and front operations.


Fig.5 Patient J., 22 years old. Dysplastic scoliosis IY degree.
At the top - before the operation, at the bottom - 5 years after the operation.
Operational incision with rear access is on the middle line of the body. Various systems of metal rods are used, which hooks or screws (t. N. Screws) are attached to the spine and then stretch it in large areas. For better stabilization of the entire design, the rods have transverse connections. Immediately after the operation, mobility is lost in fixed spinal colors. This contributes to the emergence of splicing of vertebrae bodies into a single bone block.




Fig. 6 Patient L., 15 years old. Dysplastic scoliosis IY degree. Photo and radiographs before and after surgery.
The fact that the spine on large areas is immobilized and the overall mobility of the spinal apparatus is not limited to the lack of method. During the examination in all patients having structural scoliotic arcs, complete immobility or tugaulility in the arcotted joints throughout the spine lesion scoliosis are determined. The operation only restores the spine axis and the position of the vertebrae, eliminates the compression of the spinal cord and its formations, restores the shape of the body and its physiological bends. Externally, it is practically impossible to determine that the operated part of the spine is still, since the volume of slopes of the body is maintained due to bending in the hip joints.


Fig. 7 The same patient, in the photo - stands, bent forward. Changes in the chest, left - before the operation, right - 5 years after treatment
When the front access operation, the incision is made along the edge. In this case, one edge is removed and used later in crushed form as its own bone material for fixing. It will be entered in the space between the vertebrae instead of remote disks. After opening the thoracic and abdominal cavity, the spine is released so that the surgeon has free access to the vertebrae and intervertebral discs. For correction in certain segments, discs and side drives are removed into corrected vertebrae. They are connected by a rod and after the correction is attached to it. The prepared bone material is introduced into the location of the disks. With a modern method, two rods are used for better stability if it allows the state of the spine. The disadvantage of this technique is the opening of the abdominal and chest cavities. In addition, it is sometimes necessary to wear a corset after the operation to be used to consolidate the result.



Fig.8 Patient I., 15 years old. Dysplastic scoliosis of the III degree. Radiographs before and after surgery.
The rear-access operation today usually does not require the final wearing corset, but without additional resection of the rib hump, its results in the cosmetic plan are insufficient.
The total risk of operation in idiopathic scoliosis in German data is determined by about 5%. Possible complications - inflammation of respiratory organs, respiratory limit, repeated bleeding, injuries of the nervous system. For example, in Germany it is believed that in large operational centers the risk is defined as very moderate and operations proceed relatively without complications.
The success of surgical treatment is achieved in the formation of an extended bone block along the entire length of fixing with metal structures, for which, throughout the scoliotic arc, intervertebral joints are destroyed, the bone is cleaned and the bone plastic is cleaned. A long bone battle is formed, "reinforced" metal capable of carrying out the support and protective function of the spine. Options using hook "guides" or "growing" structures without replacing them to "fixing" are doomed to failure. Upon contact of moving metal implants with bone, either resorption (destruction) of the bone or the fracture of the retainer can occur. More often due to the development of fatigue stresses, the retainer breaks and its component parts migrate in soft tissues, overlook the skin, cause pain.




Fig. 9 radiographs and photos of the patient Sh., 18 years old. Dysplastic scoliosis IY degree. Status after scoliosis correction LSZ fixture. On radiographs on the left - the fracture of the left rod of the retainer at the level of the lumbar vertebra. Silk rod shifted down by 10 cm. In the photo - at the level of the sacrum on the left, the end of a broken rod is visible above the soft tissue level. On the radiograph of the right - the same patient after removing the broken implant and fixation of the USS design
Scoliosis and pregnancy
As a rule, pregnancy does not worsen the course of scoliosis and does not lead to an increase in curvature. From the point of view of objects, scoliosis does not have any influence on pregnancy and childbirth. But this does not apply to 100% to the operated patients. Due to the strong immobilization of the lower spine, it is possible to difficulty the reaction of the pelvic ring.
Scoliosis and Army
For the citizens of the Russian Federation, the issue of call is solved on the basis of the Decree of the Government of the Russian Federation of February 25, 2003 No. 123, according to which:
The degree of scoliosis is determined by the X-ray radiograph based on the measurement of the corners of the scoliosis: I degree - 1-10 degrees, II degree - 11-25 degrees, III degree - 26-50 degrees, IV degree - more than 50 degrees (according to V. D. Chaklin) .
The angle between the two lines carried out through the center of the most rejected vertebra and through the center of the nearest unchanged one is measured. Scoliosis can be a C-shaped (with one arc of the curvature), there may be an S-shaped (with two arcs of curvature) and σ-shaped (with three curvature arcs). In this case, the severity of the state is determined by curvature with the highest angle of rejection of the spine.
Conscripts, who, on this scale, only the degree are subject to call in the Armed Forces of the Russian Federation. In addition, conscripts with I do not accept the degree of scoliosis for the category A-1. Exemption from the call in the Armed Forces of the Russian Federation (category "B") is given under the II and subsequent degrees of the disease.
- In the preparation of the material used their own materials, materials of sites www.ru.vicepedia.org and www.narmed.ru
Scoliosis is rather common pathology, known since those times when a person began to walk straight.
As a result, he appears and how to deal with him - the question that has not lost the relevance in the 21st century.
Especially the mysterious group, referred to as the term "Displanic scoliosis".
Why do children overtake the processes deforming and twisting their spine?
How can modern parents be faced with?
About pathology
Dysplastic scoliosis is the most heavy of the vertebral damage forms, due to the dysplasia of the lumbar-sacrive department.
Acquaintance with scientific terms denoting the problem helps it is better to understand the essence of the pathological process:
- Vertex dysplasia- A generalizing concept used to designate the options for its vicious development.
- Scoliosis - curvature of the spine in the frontal plane, combined with the rotation of the vertebrae.
- Dizrafia - Lack of fasting (literally). The overall designation of the innate unction of the components of the spine.
- Dismelia - Lack of organ.
- Spondylolysis - Defective gap between the joints of the vertebral arc.
- Lumbalization (Synonym Lubbarization) - an increase in the number of lumbar vertebrae due to the Agnesia Xii edges. The pathology option is not blocking I and II of the sacrum vertebra with iliac.
- Sacralization - Anomalous identity of the lower lumbar vertebra is a sacrament - blocking the transverse process of the fifth vertebra with a iliac bone, or a complete fire.
- Spina Bifida. - The incoming of the spine canal due to the violation of the merger of the arc or bodies of the vertebrae.
The history of the existence of the disease
The first famous vertebrologist who studied scoliosis was hippocrate. He believed that this pathology is the result of muscle equilibrium. The equilibrium was restored by pulling the body synchronously with pressure on the hump. The method existed until the XVI century.

Combined therapy mobilizes, correct the spine and holds the correction.
Little patients prescribe gypsum cribs, quartz irradiation, bathtubs, massage, gymnastics.
Children who came out of the youngest age group, we will add wearing orthopedic corsets.
The method proposed by Chaklin.
It is based on pulling the body against the background of creating corrective curvature.
Payment method
The compensation method includes periods of treatment:
- Mobilization with exercises aimed at strengthening the muscles of the back.
- Fixation by a long wearing gypsum corset. It is superimposed when the patient stands. At the same time, stretching on the loop of the glisson.
- Stabilization. Gypsum corset replace removable. The compensated state of the spine is supported by exercises. In case of instability, surgical intervention may be required.
Surgical intervention
Operational treatment of spinal curvatures is shown in scoliosis II - IV degree, against the background of the progression of the main pathological process.
Most common methods:
- Wedge-shaped vertebral bodies in the thoracic spine in combination with rear spondylodez with scoliosis III - IV degree by Kazmin;
- Fixation of the spine according to Chaklin;
- Discotomy in the thoracic spine in combination with rear spondylodez by Kazmin;
- Mobilization of the thoracic spine on Harrington;
- Epiphysieres of vertebrae bodies in young children in Zaprevsky;
- Wedge-shaped vertebrotomy with heavy forms of kifoscolyosis in Tsivyan;
- Tenoomyptocapsulotomy on Schurutko with scoliosis II - III degree;
- Recreation of an additional wedge-shaped semi-change in Bairov.
None of the methods correct the deformation completely. They reduce the angle of curvature, stop the progression of curvature.
LFK, Massage
Gymnastics in systematic classes forms muscles that can resist deformation. With medical workers, the complex is only being studied, the execution technique is being implemented.
Symmetric gymnastics - the main complex of the LFC. His task is to strengthen muscles subject to less load. The exercise session should be at least 20 minutes. They must be carried out systematically (2 times a day) - without skipping.
Swimming is shown at any degree of deformation. It strengthens the muscles well, contributes to the unloading of the spine, improves the functions of respiratory organs.
Massage principle - Stretching and relaxation of stress, shortened muscles of the back on the side of concreteness and toning, stimulating weakened, stretched muscles on the side of the convexity.
Video: "Massage with scoliosis"
Treatment at home
At home, the entire load on the treatment of gymnastics, the creation of the appropriate working and recreation conditions, compliance with the prescription of the doctor lies on the shoulders of parents of the sick child. Therapeutic events with the wearing corset, the LFC is durable and tedious. But the health and further life of the child depends on the carery of appointments of the doctor.
Prevention
 It is impossible to ensure the prevention of congenital changes in the bone skeleton of unclear etiology.
It is impossible to ensure the prevention of congenital changes in the bone skeleton of unclear etiology.
All events should be directed to early detection of pathology and preventing its progression.
Prevention is shown:
- Proper nutrition
- Selection of furniture corresponding to the growth of the child;
- Hard bed with a small pillow,
- Medical physical education (according to the doctor's testimony).
Children with scoliosis are not recommended by physical education in the common school group. In severe cases, learning at home or in specialized boarding schools is shown.
The child is engaged in the lingerie position on the stomach. In the interruptions makes gymnastic exercises. At night sleeps in a gypsum crunch.
Forecast
The earlier the child fell ill, the greater the danger of progression of deformations. Progression The disease continues, in the absence of therapy, the entire period of human growth. Even surgical treatment does not always stop the progression of dysplastic scoliosis. Therefore, the parents of the sick child and the patient itself should be aimed at a long struggle with the ailment.
Conclusion
- the most severe pathological change in the spine. It leads to a disorder from all basic life systems of the body.
Early identification of this, as a rule, congenital pathology is extremely important. Therapy and prevention of deformation progression should be started as early as possible.! Therefore, it is necessary to participate with the child in all mandatory screening medical examinations. When identifying pathology, it is impossible to occupy an expectant position. You need to immediately turn to a qualified orthopedic doctor.
Etiology and pathogenesis of the side curvature of the spine in children to adolescents still remain the most difficult and more important section in the problem of scoliosis. In the existing classifications of spinal curvatures, the role of the nervous system in the development of scoliosis is not enough. Orthopedists in determining the etiology of desecrations pay great attention to the dysplasia of the spine. This partially caused a large percentage of idpopathic scoliosis, i.e. deformation with an unexplained etiology.
Of the 1245 patients with scoliosis that have passed through the department, 300 children (24%) were selected with a symptom complex, characteristic of a dysrafic state, and combined into a dysplastic group. In this report, we will not concern the neurogenic group of scoliosis related to siringomyelius, poliomyelitis, neurofibromatosis, myopathy, etc., and limit ourselves only to the dysplanic group.
A dysplastic group of curvature was allocated by A. A. Kozlovsky in 1927, and then the existence of it was confirmed by G. I. Turner and R. R. harmful. The cause of the development of dysplastic scoliosis The authors considered the dysplasia of the lower lumbar and sacred spine: lumbarization, sacralization, especially one-sided, oblique position V of the lumbar vertebra or its wedge-shaped form, spondylolysis, spondylolistera, defects of lumbays of lumbar and sacred verteons. In their opinion, these dysplasia weaken the base of the spine and cause the formation of curvature and anti-observation.
However, as our observations show, often with the above dysplasia of the lumbosacral spine, primary-breast, lumbly and combined scoliosis develop.
The development and subsequent progression of these curvatures cannot be explained only by the dysplasia of the lumbly-sacred spine. This was the reason for identifying other reasons caused by the development of most severe scoliosis. For this purpose, a group of children with scoliosis were studied, in which changes were found in the nervous system, combined with the dysplasia of the lumbosacral spine.
R. R. It is harmful in 1931 indicated the possibility of a combination of the defects of the spine with dismalia, i.e., with a violation of the normal development of the lower spinal cord, as a result of which innervation disorders appear on the periphery both in the motor and sensitive sphere.
On the ability to combinations of the definition of the spine and spinal cord Other authors were also indicated (P. P. Kondratyev, E. Yu. Osten-Saken; V. S. Zubkov, A. V. Zenchenko, D. S. Fututor, V. A. Sturm, V. P. Zhigigyn, and others .). The possibility of a combination of vicious development of the spine H nervous system is due to disruption of the embryogenesis of the spinal cord and the spine coming in an inseparable interconnection and unity.
In 1909, Fucks described the characteristic splitting syndrome of the lump of lumbays-sacral vertebrae, combined with a defect of lumbly-sacral segments of the brain spinnogo. He considered these neurological symptoms and a gap in the spine vicious development of the spinal cord.
Bremer expanded the concept mielodisplasia, Fucks, and included the dysplasia of the seine-thoracic spinal cord, calling the entire snumpomplex with a disraphic state-disorder of the formation of a medullary tube. The improper formation and closure of the rear seam leads to the unclipment of the central channel and the deviations associated with these deviations from the normal development of the various structures of the brain spine.
The signs of the dysraphic structure of the BREMER body attributes the anomalies of the sternum (funnel-shaped or groove), kifoscoliosis, lengthening the upper parts of the body, a kind of curvature of the fingers, the different amount of the mammary glands, the sensitivity disorders, more often segmental type, acricyanosis, urine incontinence, often in combination with the splitting of the vertebrae .
Along with this, degenerative signs are revealed: a high solid sky, anomalies of agriculture, improper development of teeth.
S. N. Davidenkov with employees, D. S. Fututor established additional features: deformation of the spine, the arachnodactylum, the deformation of the skull, the deformation of the stop in the form of various kinds of circulators, changes in reflexes, trophic ulcers in the footsteps.
D. A. Shamburov on a large material allocated a number of additional features of the dispriephy; Some of them were family character. The most frequent were defects in the development of the bone apparatus: defects of the arms, transitional vertebrae lumbly-sacral nineteenth-region, added ribs, underdevelopment and incomplete vertebrae merge, blocking bodies and arms of the vertebrae. The limbs revealed sixpace, split or filling the phalanx of the fingers, the absence of end phalanx on one or more fingers, usually a pa clatter, the vius deformation of the joints (ankle, shoulder), the thinning and shortening of the bones of the limbs on the one hand, the Sindacticity is complete or partial.
Based on numerous clinical observations, we highlighted a distinct group of patients with a dishraphic state syndrome, in which the signs of disrapure do not bear the nature of monosimptom. Usually they are detected in the form of different complexes and in various degrees of severity of individual signs.
We have studied 300 children aged 7 to 19 years old with dysplastic spinal reverse; 88% of children were between the ages of 12, 19 years and only 12% - from 7 to 12 years. The degree of scoliosis was determined by the value of the angle measured by the Cobb method. Indications for operation were determined to a large degree of scoliosis. A curvature with an angle of from 50 to 20 °, II degree - from 21 to 40 °, 111 degrees - from 41 to 60, IV degree - from 41 to 60, IV degree - from 41 to 60 °, 111 degrees are 61 ° and more.
Dysplastic scoliosis, as well as scoliosis of any other etiology have a different propensity to progression. However, most of them relate to rapidly progressive, as 2 years after their primary detection, they achieved III and IV degrees. The development of primary breast and lumbar scoliosis can be explained only by the dysplasia of the lumbosacral spine.
The neurological examination conducted in 286 patients with various neurological symptoms in a distinct form. The asymmetry of reflexes with one-sided decrease or fraction of them was found in most patients.
The most often revealed anisanflexcy of the blade reflexes. More than half of the patients, the decrease in the reflex is marked on the convex side of the curvature. The asymmetry of the knee reflexes was observed in 124 patients, Achilles in 95. The asymmetry of tendon and periosteal reflexes on the upper limbs had 133 patients.
The greatest interest is the analysis of the asymmetry of abdominal reflexes with one-sided decrease in either the fallout revealed in 160 patients. We managed to establish the dependence of the level and nature of the curvature from falling out or reducing abdominal reflexes.
With the lumbar localization of the primary curvature, the unevenness of abdominal reflexes is most often obstacled (in 70.5%). With S-shaped scoliosis, abdominal reflexes was observed in 51.5%, and, unlike other location of curvature, the decline or loss was more often on both sides. In the primary-lumbar scoliosis, the anzoreflexia of abdominal reflexes was revealed by 29.7%, and with infantry only at 20.13%. The described asymmetry of reflexes was observed in various combinations.
A similar dependence of the direction of the arc scoliosis is established in relation to the zone of pain hypalgesia, which was segmental in nature and detected in 12 patients. Sensitivity disorder In all patients was determined at the level of the thoracic and cervical segments. The hypalgesia zone with one-sided falling always coincided with the convex side of the scoliosis, and with S-shaped scoliosis in 3 patients, sensitivity disorder was revealed from both sides.
These data almost completely coincide with such a combination of scoliosis, sensitivity and anneflection disorders in children with Siringomyelia.
A. A. Kozlovsky, G. I. Tourner, R. R. It is harmful, describing dysplastic scoliosis, believed that the asymmetry of the lumbar spine causes the inclination of lumbar vertebrae, followed by the development of infancy. Our observations have shown that out of 300 children surveyed primary lumbar curvings were only 17% (51 children), lumbar-thoracic in 25% (75 children), and primary-breasts v 58% (174 children). Thus, in the majority of patients with the dysplasia of the belt, the spine were not primary-lumbar scoliosis, as A. A. Kozlovsky believed, G. I. Tourner, R. R. is harmful, and primary-thoracic.
In terms of gravity, primary-breast scoliosa again occupy the first place. Scoliosis III and IV degrees among them met in 59.5%. Primary-lumbar scoliosis belongs to the number of the most benign; Most of them (58.83%) were 1-11 degrees. As you can see, most severe scoliosis occurs among the primary-chest, and not among the primary lumbar scoliosis.
In 30 patients, various degrees of atrophy of the sizes are noted. Most often among them, atrophy of small muscles of brushes, supreme muscles of the thigh and lower legs were revealed.
Muscle hypotension, especially on the limbs, was observed in all children with dysplastic scoliosis, but varying degrees of severity. As a result of hypotension, the amplitude of movements in the knee, elbow n radiation joints increases. It should be noted that with the age of hypotension decreases sharply or disappears completely.
Different vasomotor-trophic violations: acricyanosis, marble and cooling limbs, increased sweating, sharply expressed white dermographism on the legs, reaching the character of the "drain", are observed almost in all patients.
Less often in children with dysplastic scoliosis occurs hyperitrihosis in the field of the sacrum and along the spine, the skin pigment disorder in the sacral region, rudimentary supplemental nipples, fastening of the skin in the integration region, shortening and refinement of bones, more often on the one hand. In 15 children, in addition to the listed symptoms, revealed congenital nastagm, signs of spinal lesion in the form of hyperreflexes, clone stop, pathological reflexes.
Along with neurological symptoms, the children of this group observed the deformation of the skull (hydrocephalic or tower), 80% met a high vaulted sky, stop deformation (hollow, occasionally flat foot). In 35 girls, the asymmetry of the mammary glands is marked, sometimes very significant.
In 54 patients, spnder disorders were revealed in the form of a violation of the function of the pelvic organs. Night incontinence of urine persisted in children from 3 to 17 years, and 16 of them had a night incontinence of urine, relatives suffered. In 38 children out of 54, the violation of the function of the pelvic organs was combined with different spinal bone dysplasia. In 32 of these children there were defects of the foreman of November and sacral vertebrae, and 9 they captured at least 2 vertebrae, all the sacres of the vertebrae, and 1 patient had a spinal out hernia. In 6 other patients there were transitional lumbly and lumbosacious verteons.
The level of scoliosis in these patients maintained the former pattern. Most had pectoral scoliosis (26 patients), the second place was occupied by lumbar (17) and the minority of patients (11) were primary lumbar scoliosis. Primary-lumbar scoliosis in this group of patients belonged to the easiest.
X-ray examination conducted by all patients found various bone dysplasia in 222 of them (74%). The defect of the alpine-sacral vertebrae is discovered in 159 patients (71.5%). In 14 patients, the defects were combined with other spinal defects: spondylolisthesis, sacralization, lumbish, added ribs, spondylolysis. In one group of patients (10 children), the arc defect has a kind of oblique or transversely located narrow slit; In 25 patients, there was Spina Bifida Aperta with a defect of the foremen from 0.3 to 0.8 cm, and one of them had a spinal out hernia. In the rest of the patients, the defect of the forehead was combined with their mixture, as a result of which both half the arrangements were located at an angle or each other.
Comparison of the data obtained during the examination of patients, with literary instructions and with the detected neurological and other congenital symptoms, suggests that the splitting of the forehead in our patients is one of the symptoms of disrapure.
In 63 patients, transitional vertebrae was revealed, 9 - various worshipers of developing ribs. Sacralization was found in 35 children, and one-sided only 3. In 4 patients, sacralization was combined with other spinal defects. Lyumbalization was revealed in 19 patients, one of them is one-sided only 5. In 7 patients, the Lumbali was combined with other spinal dysplasia.
The underdevelopment or absence of XII pairs of ribs (11 thoracic, 6 leafy vertebrae, 11 pairs of ribs) were revealed in 10 patients. We believe that such pathology occurs significantly more often, but due to the fact that they do not count all the ribs, they are related to lumbalization.
In 18 patients, in addition to the neurological symptoms and bone dysplasia, there were other defective defects, often multiple: solid sky splitting, head of the finger brush, radioline synostosis along with partial giant of three fingers on both feet and rudimentary supplement nipples, congenital abstruse muscles with One side, a diaphragmal hernia, hip dislocate, cervical varetle deformation, Krivoshoy, shortening and refinement of bones and many other congenital development defects.
These observations, although few in the general group of patients talk about the great prevalence of congenital defects for the development of children with DPSlastic scoliosis.
All the symptoms identified in children with dysplastic scoliosis fully correspond to the described clinical, radiological neurological symptoms of disproph status. And in our patients neurological symptoms are of the greatest interest. which. As we believe, the reason for the development of scoliosis.
The dynamics of neurological symptoms, traced in the 30 of our patients with a dysplastic form of scoliosis for 2-5 years showed the immutability of the primary identified symptoms with an increase in scoliosis. This indicates independent of the dynamics of the curvature of the existence of neurological symptoms in this group | Children.
A completely different dynamics of neurological symptoms was observed in 8 children with scoliosis, complicated spinal cord compression. They are characterized by the emergence and rapid increase in neurological spinal symptoms due to the progression of scoliosis.
The level of spinal symptoms corresponds to the level of maximum deformation of the spine. With increasing the pares, due to compression mixture, a picture of a sponal block is detected in the spinal fluid. With isotopic myelography, a partial or complete block at the level of the maximum deformation of the spine is confirmed.
Corrigative treatment of scoliosis in 6 patients with a burnt corset in combination with vitamination therapy, massage, light healing gymnastics led to the regression of previously neurological symptoms with full function recovery. All 6 patients have a treatment started shortly after the appearance of compression symptoms. Only 1 patient even the operation of decompression laminectomy with the removal of the bone wedge did not lead to a positive effect, since there was a picture of severe irreversible myelita.
Summing up all the data outlined, we conclude that the polysptomic clinic, detected in children with dysplastic scoliosis, most of all corresponds to the symptom complex described by Bremer, S. N. Davidenkov, D. A. Shambururov and others. As a dysrafic status. Bone dysplasia identified in children of this group is rarely the immediate cause of the formation of primary lumbar scoliosis.
The cause of the development of primary-breast, lumbar and combined scoliosis in most children, as we believe are neuro-trophic and neuromuscular disruption of spinal origin, observed in disrapure status.
conclusions
1. Most of the 300 children with dysplastic scoliosis were primary and lumbar scoliosis, the development of which cannot be fully explained only by bone dysplasia of the lumbosacral spine.
2. In 286 children (95.3%), various neurological symptoms were revealed, combined with bone dysplasia and other malformations. Violations in the nervous system are due to the defects of the development of a neural tube, improper formation and closure of the rear seam, which is described as a dysraphic status. The detected neurological symptoms are characterized by stability, they do not increase with the progression of curvature, which speaks in favor of their primaryness.
3. Anomalies of the development of a neural tube, as we believe, lead to neuromuscular and neuro-trophic disorders, which determine the asymmetry of the growth of the vertebrae and the development of the side spinal curvature from this group of children.
Thoracic Surgery - Surgery.su
Scoliosis D.spoil- the most severe form of spinal curvature with anomaly of its development, resulting from the dysplasia of the lumbosacral spine. At the beginning displastic scoliosis It may well not give out her anise. The deformation is detected in children aged 8-10 years and tends to steady progression. The occurrence of it is associated with the anomaly of the development of V of the lumbar and I sacral vertebra. What, apparently, is explained by increasing the level of load taking place as the organism's development and development. In cases where the scoliosis remained unrecognized, the process progresses (more noticeable with the damage to the breast, and there are certain complications.
For dysplastic scoliosis, the development of large compensatory opponation arcs in the thoracic spine, accompanied, as a rule, with a sharp torcia of the vertebrae bodies and the formation of a gentle rib ribbin, in which not only twisted ribs take part, but also the acute processes.
One of the consequences of the dysplastic scoliosis is the formation of the so-called re-rob, which is a displacement of the ribs, especially noticeable when the patient is tilted, that is, in a bent position.
To eliminate this deformation, it is necessary to first eliminate the scoliotic curvature of the spine. Only when the latter takes a normal form, it will be possible to talk about alignment and returning to the place of pathologically modified edges. However, it should be clearly aware that the ribs are not so plastic to eliminate the defect quickly and on it all one hundred percent - it will have to work seriously and stubbornly.
A person has a skeleton formation ends with thirteen-sixteen years. Upon reaching this age, it is impossible to eliminate the scoliosis, and therefore the roiter hump, the conservative methods will not work - it will be necessary to need an operation. That is why it is very important to establish the presence of this problem in a timely manner and apply for the fight against it to the specialists of the appropriate profile, which will develop with the participation of the parents to normalize posture in the patient of the child.
Among the procedures that contribute to the elimination of the rib hump, we can note the wearing a special corrective corset, which allows to reduce the load on the spine and prevent even greater deformation of the skeleton. It is selected and used exclusively under the supervision of an experienced specialist in combination with therapeutic massage, gymnastics and breathing exercises. That's right, individually, a selected complex of physical exertion also has a stabilizing effect on the spine, strengthening the muscles of the body and speeding up the correction process.
Dysplastic scoliosis is a side deformation of the spinal column with a disorder of metabolism and blood supply in the oil-butter tissues and the rotation of the vertebrae in the vertical plane (rotation or torsion). Most often, the disease appears at 3 years old. Significantly less often displaced lateral curvature in children 5-6 years.
Displanic disorders are determined with the external examination of the child. A typical manifestation of the disease, starting with 1 degree, becomes the roar hump. With it, the deformation of the chest and the ribs, which increases with the slope of the person ahead. This anatomical feature of the disease significantly complicates the treatment process.
To eliminate curvature, it is necessary to work not only over the return of the vertebral axis to the correct position, but also on the elimination of respiratory and heart failure. Due to the displacement of the internal organs from many effective exercises of a complex of medical gymnastics, it is necessary to abandon with dyslastic curvature.
A disease is formed against the background of the displays of the sacroist-lumbar vertebral pillar. Dysplasia - impaired anatomical form and structure of the body.
When changing the vertebrae, the vertical axis is disturbed and a primary scoliotic arc is formed. As a rule, it is localized in the region of the lumbar-sacrive department. Over time, the deformation progresses and leads to a number of serious consequences:
- Infringement of nerve roots with pain syndrome;
- Spinal cord compression with immobilization of limbs (paralysis, paraplegia);
- Mental disorders (reduction of memory, attention);
- Specific curvature of the fingers of the foot (segmental acricyanosis);
- Frequent night urination;
- Uneven tendon reflexes on both sides of the body (knee, achilles);
- Vasomotor disorders (blood pressure jumps, local redness of the skin).
Segmentary acricyanosis is accompanied by local curvature and the formation of individual fingers of the foot (depending on the implanted nerve). 
The cause of the formation of pathology is congenital vertebral abnormalities:
- Lumbalization is an instance of V lumbar with I sacral vertebra (L5-S1) with the formation of a clear boundary between the lumbar department and a sacrum in the form of an intervertebral disc;
- Sacralization - L5 firmly grows with a sacrum without explicit signs of differentiation;
- SPINABIFIDA - Complete uniqueness of the arms of the vertebra.
Pathology is characterized by a sharp torica of the vertebrae with the formation of compensatory secondary arcs in the thoracic department. Ribs and ostic processes are involved in their education during the deformation of the chest. This reduces the life capacity of the lungs.
In such a situation, the "twisting" of the vertebrae, a scoliotic arc to the right or left, as well as a decrease in the height of intervertebral disks is traced in such a situation.
These changes lead to an increased hypermobility of the joints of the spine and weakness of the muscles of the back. In the lateral curvature in the lumbar section, the muscles of the pelviotrohythnic group (buttocks and the small pelvis) arise.
With dysplastic deformation of the spine 1 degree, the following treatment methods are applied:
- The deformation of the 1 degree is effective in swimming the style of Brasss within 3 months of regular training. In specialized healing groups of the instructor, the style of swimming is selected individually depending on the characteristics of the pathology.
- Massage is carried out in combination with other methods of treating pathology. It relaxes a skeletal muscles and stimulates blood supply.
- Therapeutic gymnastics is the basis for eliminating the deformation of the spine. The set of exercises with scoliosis 1 and 2 degrees of doctors are selected only after a careful examination of the patient.
- Normalization of the diet in the lateral curvature of the spinal column is carried out in order to eliminate the obesity and restoration of physiological metabolism. It is also necessary to ensure the qualitative flow of nutrients into intervertebral discs.

The diet with the right-sided or left-sided curvature of the spinal column involves the refusal of greasy and canned products. Daily diet should be included dairy products, fish and olive oil.
- Electromability helps to remove muscle "clamps" and normalize skeletal muscles tone. The method is used in large medical clinics.
- Wearing an orthopedic corset allows you to reduce the load on the spine and prevent the progression of deformation. The product is selected by an orthopedist or traumatologist.
When deforming the spine 3 and 4 degrees often have to use surgical techniques.
Surgical operations in the side deformation of the spine
Operational treatment of scoliosis is characterized by a high risk of complications and consequences. It is embezzlened only when the angle of curvature of a scoliotic arc is exceeded over 40 degrees.
Indications for the operational treatment of vertebral dysplasia:
- Strong pain syndrome, which is not removed by conservative means;
- Fast progression curvature;
- The angle of curvature is over 60 degrees;
- The pronounced cosmetic defect of the back (at the request of the patient).
It should be noted if the angle of curvature is more than 60 degrees, the state irreversibly leads to the formation of cardiac and pulmonary failure.
The main objectives of surgical interventions during the deformation of the spine:
- Elimination of cosmetic defects;
- Elimination of curvature;
- Removing compression syndrome;
- Prevent damage to the spinal cord.
Prevention
Dysplastic scoliosis of 1 degree can be effectively treated conservatively.
Prevention of dysplastic scoliosis includes the following principles:
- Regular stay in the fresh air;
- Long-term foundation in a horizontal position on a solid surface;
- Compliance with the correct posture;
- Physiotherapy.
Regular outdoor walks improve the metabolism and help to provide tissues sufficient for the normal functioning of oxygen cells.
Stay on the horizontal shield is recommended for patients with pain peeling syndrome. The method is quite effective, but is accompanied by psychological discomfort from the patient. To withstand the 2nd weekly lying children is quite difficult.
Compliance with the correct posture is a necessary condition for the formation of a physiological vertebral axis. Very often, at 1 degree of pathology, the normalization of the position of the back during seating, lifting weights, physical exertion allows to eliminate the pathological curvature of the spinal column.
Therapeutic physical culture has a stabilizing effect. With it, you can quickly achieve the correction of the spinal column. LFC can be used not only on 1 and 2 stages of pathology. It is prescribed a month before the upcoming operation with scoliosis 3 and 4 degrees, as well as at the patient's rehabilitation phase.
In conclusion, I would like to remind readers about some important principles of healthy spine development:
- If you are still sitting for more than 20 minutes, you should take a break in work and move a little;
- Frequently change the position of the legs at the desk at the desk (put the feet together, and then dug them. Place the socks of the duck and knutut);
- Put your hands on the armrests of the chair to remove the burden on the spine;
- Tighten your knees to the chest.
When performing morning gymnastics, try to get back to the back to eliminate the vertebral dislocations.
Scoliosis displays quickly progresses, so "to do" them should immediately after detection.
Among the pathology of the spine, various curvatures are often found. Normally, the axial skeleton has some physiological bends designed to provide an amortization function. But the improper distribution of the load leads to the emergence of pathological conditions - kyphosis, lordoses and scoliosis. The latter are widespread among school-age children. And the most striking representative of this pathology consider S-shaped scoliosis. Why the spine becomes curves and what to do for his straightening, you can find out after consulting a doctor.
General
Scoliosis is called the deformation of the spinal column in the frontal plane. If curvature has two arcs facing different directions, then called S-shaped. The first, as a rule, is in the thoracic department at the level of TH7-TH8, and the second - in the area of \u200b\u200bthe belt (L1-L2). Most often they are unequal. The higher the scoliotic arc is located, the faster the pathology progresses. And the presence of lumbar bending significantly aggravates the deformation of the inflation.
Primary arcs provoke the appearance of secondary, so the back becomes more curve. If both bends are developing in parallel, then they balance each other. In addition, a rotational displacement is observed - the spine slightly turns around the central axis. This is compensatory, due to changes in the position of the center of gravity.
The reasons
The appearance of scoliosis is mainly due to external reasons. Basically, its development is characteristic of children's and adolescence, when the posture is disturbed at the seat at the desk or table. The spine at this time is very pliable and quickly responds to change the load.
There are innate cases associated with dysplastic processes in bone-cartilaginous tissue, as well as vertebral anomalies. Then scoliosis is diagnosed in children after 1 year. Often, similar changes are associated with Rakhit - vitamin D deficiency at an early age. And the appearance of the spinal curve in adults is due to the following states:
- Osteochondrosis.
- Intervertebral hernia.
- Osteoporosis.
- Osteomalacia.
- Stenosis of the spinal canal.
- Osteomyelitis.
- Tuberculous spondylitis.
- Tumors and metastases.
- Consequences injuries.
- Transferred operations.
With degenerative-dystrophic pathology, a reflex muscle spasm is often observed, which can lead to the appearance of pathological bends. The same thing happens if bone tissue is destroyed or connecting spikes are formed.
If there are risk factors, you need to be examined in a timely manner at the doctor, since the solar curvatures are very difficult to corrected and are able to significantly limit the active life.
Symptoms

Contrary to popular belief, scoliosis is accompanied not only by external signs and is not only a cosmetic defect. The spin curve is a precursor of serious health problems that appear in children and progress in adults. At the same time, the manifestations of scoliosis are entirely dependent on its severity. The classification of pathology is based on the magnitude of the angle of the primary arc located in the thoracic department. Therefore, S-shaped scoliosis may have several degrees:
- The first is the angle does not exceed 10 degrees.
- The second - angle reaches 25 degrees.
- The third is an angle value of 25-50 degrees.
- The fourth is an angle of more than 50 degrees.
It is this feature of scoliosis that is based on clinical diagnostics and determine the picture of the disease. And if the initial stages have scarce symptoms, then moderate and severe forms are accompanied by severe structural and functional changes.
Scoliosis 1 degree
In the early stages of development, pathology is minority. S-shaped scoliosis of 1 degree may not be detected and regarded as some constitutional feature. But at the same time, it is accompanied by well-defined manifestations, which include:
- Slouch.
- Released shoulders.
- Ollowing head.
- Different level of adrenal and blades.
At this stage, there is one arc located in the thoracic department. Muscular roller is palpable from her side. An important diagnostic feature is the disappearance of the deformation in the situation lying. If the load does not stop, the curvature increases.
Unfortunately, the first degree of scoliosis is often skipped. Namely it is the most favorable for correction.
Scoliosis 2 degrees
S-shaped scoliosis of 2 degree becomes more noticeable. The side displacement of the spine does not completely disappear when the load is eliminated, since already has partial fixation. The symptoms of the previous stage are aggravated and new ones appear:
- It is planned by the roar hump - one-sided penetration of the chest.
- A secondary arc is formed at the level of the lumbar department.
- The asymmetry of the triangles of the waist.
- The vertebrae deviates along its own axis.
Changes at this stage are partially reversible, so it is impossible to allow further progression of scoliosis.
Scoliosis 3 degrees
This degree of scoliosis is accompanied by a pronounced deformation of the back and chest. There is a deviation of the body toward the primary arc. The lower ribs can concern the ridges of the iliac bones. But along with local signs, there are violations in the work of the internal organs observed during the load:
- Pulse care.
- Feeling of heartbeat.
- Dyspnea.
Such phenomena are associated with hypertension in the pulmonary circle of blood circulation and create additional restrictions for physical activity.
S-shaped scoliosis of 3 degrees is accompanied not only by pronounced changes in the axial skeleton, but also impaired heart function and lungs.
Scoliosis 4 degrees
The last stage of scoliosis has the most severe manifestations. The back is strongly curved in the direction of the main arc, the ribs can even dive even in the cavity of the small pelvis. For the clinical picture, the following signs are characteristic:
- Pain in the spine.
- Cardiopulmonary failure.
- Weakness in the limbs.
Sometimes pronounced spinal disorders are developing in the form of paresis and paralysis. Such a state leads to a significant limitation of human functional abilities, becoming the cause of disabilities.
Treatment

To align the back curve during scoliosis, a hard and long-term treatment is required. It includes conservative and operational techniques. The choice of each method depends on the degree of curvature and its progression. Do not think that the initial signs of scoliosis do not require correction - the turn, it must be started at this stage. In this case, the effect of treatment will be maximal.
To help in the treatment of scoliosis, you need to try to eliminate those factors that predetermined its development. It is necessary to achieve the correct distribution of the load on the spine, so as not to increase the deformation. Children are engaged in a smooth posture from the very beginning of classes at school. It should not sit at the desk for a long time and wearing heavy briefcases in one hand. And sleep better in the half-row mattress.
In addition, attention is paid to healthy nutrition, which should contain all the necessary substances, especially vitamins and calcium. Daily occupation should be the morning gymnastics and outdoor walks.
Conventional activities are aimed at the full development of the child's muscular and skeletal system and complement the main treatment of scoliosis.
Medical therapy

The spinal curvature often requires the appointment of medicines. This is due to the need to reduce unpleasant symptoms and improve metabolic processes in the musculoskeletal system. For this apply the following medicines:
- Non-steroidal anti-inflammatory (Ksefokam, Dikloberl).
- Miorosanta (Middokalm, Tolperil).
- Vitamins (Milgamma, ascorbic acid).
- Calcium preparations (calchecin).
If disorders are observed from the chest organs, cardiac drugs, antispasmodics or other means may be required. Each drug is appointed only by a doctor, taking into account the testimony.
Physiotherapy
Gymnastics is the main method of active correction of the spinal column. Exercises for S-shaped scoliosis help strengthen the back muscles, work out the right posture, unload one departments and adjust the position of others. After classes, patients feel the improvement in overall well-being and an increase in physical activity. The following exercises are effective in the early stages:
- Lying on the stomach at the same time lift a variepete leg and hand.
- Lying on the back, lifting the legs above the floor, make the movements of the "scissors".
- Being in the same position, bend legs in the knees and make the slopes to the sides.
- Standing on all fours, sit down on the foot, resting his palms in the floor. Gradually, with the help of hands to move the torso to the sides.
- In the standing standing shift the blades with her hands lowered.
- Walking on socks with arms raised and on the heels with the "castle" on the lower back.
The program of gymnastics during scoliosis is designed individually for each patient. This takes into account the magnitude of curvature and clinical signs.
Physiotherapy

To improve the state of the axial skeleton, physiotherapy methods are applied. They help relax muscles, improve the elasticity of bundles, stimulate blood flow and biochemical processes in soft tissues. Against the background of such treatment, the correction of scoliosis will have the best effect. The following procedures are used mainly:
- Electrophoresis of drugs.
- Wave treatment.
- Reflexology.
- Electromability.
Physiotherapy is appointed by a doctor based on the age of the patient and the concomitant states.
Massage
The active treatment methods also include back massage. It is necessary to affect not only the chest and lumbar departments, but also for neighboring sites. To do this, use techniques of stroking, rubbing, pressure, kneading. Massage helps to remove muscle spastic and improve blood flow in the tissues.
Passive correction
Passive correction methods are not used as independent treatment. They are applicable only in combination with active therapy, especially gymnastics. These funds include:
- Pull out (traction).
- Gypsum corsets.
- Curving cribs.
This reduces the deformation of the spine, and to consolidate the effect it is necessary to carry orthopedic orthoses.
Conservative measures have a pronounced effect only at 1 and 2 degrees of scoliosis, and in the future they are considered as preparation for the operation.
Operation

The most radical treatment of S-shaped scoliosis is an operation. Surgical paths perform the mobilization of the spine and reduce the deformation. For this use the following techniques:
- Recreation of ribrone processes.
- Front and rear spondylodez.
- Installation of distractors - fixtures for stretching (sliding).
- Decompression of nerve roots.
Operational intervention warns the progression of deformation, but often ends with almost complete immobilization of the spine departments. Therefore, its prevention is considered to be the most effective means of combating scoliosis, early detection and adequate treatment of initial stages of pathology.